|
Correction of
scoliosis in adulthood without surgery Andrej Gogala Slovenian
Museum of Natural History, Prešernova 20,
Ljubljana, Slovenia; e-mail: agogala@pms-lj.si Introduction |
|
|||||||
|
|
At seven
or eight years at home. I wear a Milwaukee brace because of scoliosis, its collar part is only seen. At the age of 11
years I stopped wearing braces because of renal disease and remained without
any other treatment of scoliosis as well. Irregular curvature of the spine
increased over the years. |
|
||||||
|
|
With children in the school of the Orthopaedic Hospital Valdoltra. |
|
||||||
Discontinuation
of treatment
Therapy restored
I found that my spine is not bent forward in the
lumbar part as a normal lordosis, it is only bent sideways. I assumed that
the curve sideways will disappear, if I managed to bend the spine forward, as
is correct. Perhaps this will also have a beneficial impact on the higher
parts of the spine as it will have to establish a new equilibrium. When I
still had a catheter, I tucked socks at the back at night under the elastic
net that held it in place. When I slept on my back, it was forcing me to arch
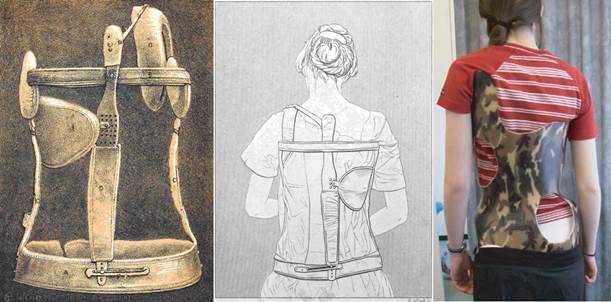
my back. Then I bought elastic bodice in a shop with medical stuff. I
stitched longitudinal metal braces to it, which I twisted in the form of my
body. The one that crossed the hump had to be bent almost at right angles to
fit it. With this corset I then went to sleep and walks. I also trained the
muscles that straightened my body. Three months later, in the spring of 2006,
I ordered an underbust corset of the waist cincher type on the internet. It was actually a band used by ladies to
constrict their waists (Axfords
C225). It forced me into an
upright posture and created lumbar lordosis. I had to take it off before lunch
so I could eat but put it on again before sleep. After some
time I ordered a longer underbust corset, which grasped the pelvis and ribs
better, but since it was not custom made, it did not fit perfectly (Axfords
C229). When I received it by
post, my mother showed me hers that was very similar, only it was laced by
the side, not the rear. She had scoliosis at a young age too and in that time
scoliosis was treated with corsets from fabric, like the one I am using now.
I walked a lot wearing the corset, also in the mountains. In any case, it is
necessary to strengthen the back muscles, so I also practised.
|
Further Reading
Scoliosis – to operate or not?
Psyche and Health
Putting on a Corset
|
|||||||
|
|
In June 2006 at a lecture. This year, at the age of 43
years, I began to wear a corset of the waist cincher kind which created
previously unnoticed lumbar curve (lumbar lordosis). This proper curvature of
the lumbar spine is diminished in scoliosis. Photo by N. Elsner.
|
|||||||
|
Shorter right
leg?
Leg length
discrepancy, as the phenomenon of uneven leg lengths is called, is usually
referred only as a cause of nonstructural scoliosis which can be corrected by
the use of shoe lift. However, when nonstructural scoliosis is not eliminated
in time, it evolves into structural scoliosis, which cannot be corrected by
posture improvement (Hawes & O'Brien 2006). In order to give the pelvis a horizontal
position while walking, I should have the sole of the right shoe two
centimeters thicker. So thick heel insoles for shoes are not available, so I
made them myself from cork. I inserted them in shoes, but after a long walk
the heel became painful and all shoes are not even suitable for such thick
insoles, so I soon gave up. For successful therapy specifically designed
shoes should be used, one of them should have a higher heel. But pelvis can
be tilted also because of rotation, which is caused by scoliosis. The
diagnosis of uneven leg lengths could be wrong. Finally, progress
When I lost hope
that I will achieve anything with the corset, I stopped wearing it. After a
few days, I was surprised to find that there has been an improvement. Thus it
is necessary to interrupt treatment with the corset to allow the spine to
find a new balance. The corset prevents that by pressure to the whole body. I found that I need a corset that would stretch all the way from the armpits to the pelvis, and press the hump in order to reduce. It should be custom made and I found a website where I could order an overbust corset made to my measures in England without too much additional charge (Corsetcurves Venus). I got it after a few days. It fits me much better, just behind the hump it is standing sideways. I wore it since September of 2008. However, a vein containing arterial blood from the fistula, necessary for the dialysis, clotted in my shoulder. I began to wear the corset only occasionally. Sometimes at night, sometimes during the day or at night and in the forenoon, only a day or two a week. On the trips I went mostly without the corset to strengthen the back muscles while walking. I was afraid that the corset could worsen blood flow by pressure and could promote thrombus formation. When I photographed myself in July 2011 and compared the situation with old photographs, I noticed a significant improvement of my back, anyhow. I noticed the same also by touch and in the mirror. So, the five and a half years of efforts had an effect. Correction of scoliosis in adulthood without surgery is possible. |
||||||||
|
|
In August 2009,
the hump was still pronounced despite a three-year therapy. Photo by M.
Maher. |
|||||||
|
Overbust corset improves body posture and
shapes the chest, but derotation is achieved only after the interruption of
corset wear. View from the side, front and rear in July 2011. |
||||||||
|
From July
2011 until January
2012, I continued to alternate
days when I wore the corset, and days when I did not. The corset improved the
position of the ribs and arched my back, but it could not decrease vertebral
rotation, and therefore did not reduce the hump immediately. But perhaps it
softened ligaments, so I can, after I take off the corset, by pressing the
hump from behind and with contractions of the back muscles, decrease slightly
the hump, moving the vertebrae slightly towards the correct position.
Comparison of images taken in July and January documents a substantial
improvement. In side view from July, the hump was of a semi-circular
shape and connected with the back at right angle. The skin of the chest and
abdomen at front was loose, not supported by the ribs. On 10th
January the back was evenly narrowing towards the waist. At front, ribs
supported skin of the chest and abdomen. |
||||||||
|
The left image was taken in the first of
July 2011. Although I had already reduced the hump, it still looks horrible.
It is of a semi-circular shape and connects with the back at right angle. The
skin of the chest and abdomen at front is loose, because it is not supported
by the ribs. Right view was created in the 10th January
2012. The difference should be obvious to everyone. From the blade down the
back is evenly narrowing towards the waist. At front, ribs support the chest
and skin of the abdomen. |
||||||||
|
But how to convince someone on my success?
Each thinks that it is a hoax. How could I achieve the impossible in such a
primitive, Victorian way? But corsets, such as used by me, successfully
curved bones through the centuries, only that ladies used them to create
narrow waist, a beauty ideal. Initially they were used to treat scoliosis as
well, but were then replaced by more modern braces which do not straighten
the back by compression, but by supporting and extending it. The bone,
however, most effectively transforms under pressure. It is growing stronger
in those places that receive maximum stress during movement of the body (Pearson
& Lieberman 2004). Good old corset, shaped after the Victorian
example, achieves success by putting load on the ribs and vertebrae through
them. Since it is made of cloth, it is permeable to the air and moisture, so
it can be used even during strenuous walk under the hot sun, which plastic
brace does not allow. It is more comfortable as it adapts to the shape of the
body. It can be washed by hand, using soap. Spiral steel boning is now used
to stiffen it and not whale bone. The corset is not adjusted to the back
deformations, it is symmetric. The body must adapt to it, to straighten. Monitoring: March 2012
In side view, in comparison with January the hump seems increased again at first sight. But a closer examination reveals that the scapula, which was previously raised by the hump, is lowered. Ribs, which previously raised it, form the curve of the hump. But the chest and abdomen at front are supported well and not loose, as they have been in July 2011. |
||||||||
|
Comparison of the back, photographed in
January (left) and March 2012 (right). Apparent curve has been reduced and at
the left side of the body we see the ribs, which were shifted before. |
||||||||
|
Comparison views from the July 2011 (left),
January (middle) and March 2012 (right). Spatula, which was raised before,
descended lower in the right picture. |
||||||||
|
Why interrupt corset wear To determine why we need to alternate days when wearing corset
and days without it, five days in a row the
corset was worn during the day and then the back photographed.
In lateral view,
the hump was
reduced and the scapula lifted. The view from
behind showed the curve sideways to measure 144°, thus it was more pronounced than in previous image (151°).
The next day, the curve measured
151° again. Corset can thus temporarily worsen
the condition of the curve, but
this is rapidly corrected when corset wear is
interrupted. The chest easily rotates for a certain degree when the corset is
tightened too much. Then it derotates again, switching between two stable
positions. When this happens often, therapy should be discontinued for a
longer time. After the corset is taken off, derotation
forces can be applied to the thorax. Only by them, correction of scoliosis
can finally be achieved. We must press the hump from behind, not laterally as
this flattens the rib cage. Similar manipulation was performed to correct
spinal deformities already by Hippocrates and Galen. While extending the
body, they pressed the hump with the leg, whole body or with a plank,
attached to the wall for leverage (Vasiliadis
et al. 2009). But press against the chair backrest or the hard floor when
lying is sufficient. In the days when corset is
not worn the chest can expand and the muscles are more active. Besides,
intermittent bouts of loading elicit a greater response in bone forming cells
than a single long lasting bout of loading and thus stimulate bone remodeling
better. In rats, eight hours of recovery time are required to restore
the full responsiveness of cells (Pearson
& Lieberman 2004). |
||||||||
|
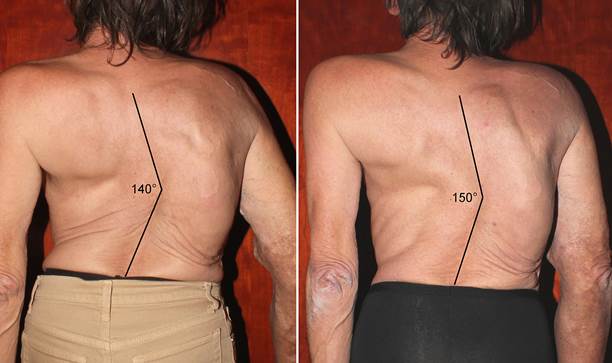
On 27th March 2012 the curve
measured 151° (left);
after five days wearing corset, the curvature
on the 6th April increased to 144° (center);
just a day later, the curve
measured 151° again (right). |
||||||||
|
|
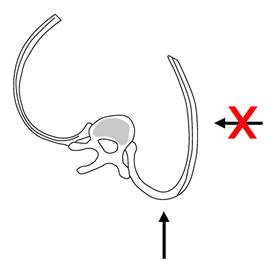
On the hump created by deformed
ribs, we have to
push from behind. Lateral pressure would
flatten the chest even more. |
|||||||
|
Towards
eradication of scoliosis?
|
||||||||
|
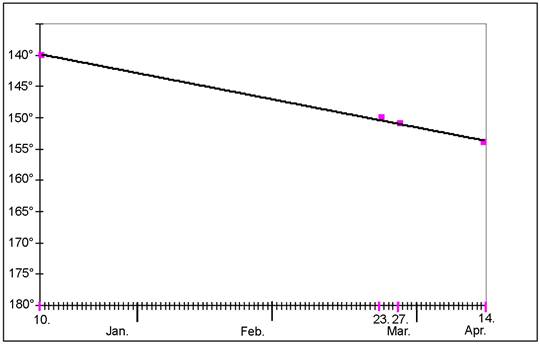
Reduction of the apparent
spinal curve from 10th January to 14th April 2012.
Through the points we can draw a straight line, so the curve steadily
decreased with time. |
||||||||
|
Apparent curvature of the
spine on 10th January measured 140° (left), 23rd March
150° (middle) and 14th April 154° (right). |
||||||||
|
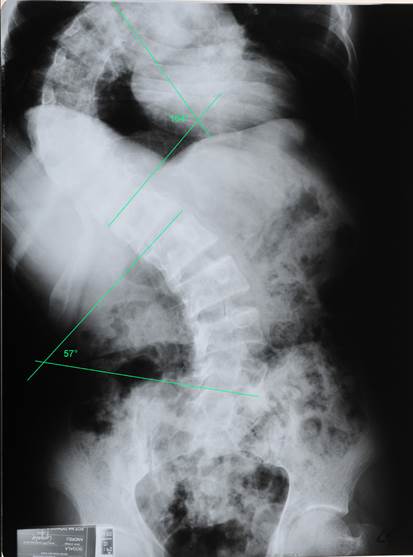
How severe is actually my
scoliosis? From the archives of the Department of Dialysis of the Ljubljana Medical Centre, I got x-ray images showing my
spine. Finally I was able to
measure Cobb angles, which are used to
measure the curvature and
to estimate the severity of deformation. In the images from the years 1997
and 2005 only the thoracic
curvature is seen which is equal in both images,
so it did not deteriorate before the
treatment. The image from 2010
shows both curves. Upper thoracic curve
is larger and measures
104°, the lower lumbar measures
57°. Curves over
60° are considered a very
severe form of scoliosis and
in the curves over
80° it comes to lung function impairment. Vital
capacity of my lungs measured 1380 ml in 2010, only 40%
estimated for my hight. Early onset scoliosis like
mine can cause larger curves than more common adolescent scoliosis because
unbalanced growth of the spine lasts longer. Usually the curvature progresses
slowly also in adulthood. Linear rate of progression at about
one Cobb degree per year had been demonstrated
in progressive adult scoliosis (Marty-Poumarat et al. 2007). If
untreated, juvenile scoliosis can cause serious
cardiopulmonary complications and premature death (Mohar 2012). Untreated
late onset scoliosis, for comparison, causes little physical impairment other
than back pain and cosmetic concerns (Weinstein et al. 2003). |
||||||||
|
|
X-ray image from 2010 with Cobb angles measured. Thoracic curve measured 104°,
lower lumbar 57°. |
|||||||
|
New improvement in June: pelvic
obliquity reduced Imaging of June 9th
showed unchanged curve of the spine, an important change from the previous
state I noticed later. I found that my pelvis is no longer tilted and
analysis of the photographs showed a significant difference. Pelvic obliquity can be the consequence of unequal length of legs,
but pelvis could also be shifted due to rotation in the lumbar part of the
spine present in scoliosis. Scoliosis can develop because of pelvic
obliquity, but scoliosis also causes or increases pelvic tilt. It is difficult to determine what occurred first. I linked the iliac crests on the photos with
a line and draw a median line of the body. Then I measured the angle between
these lines. It would measure 90° if the
pelvis was not inclined. In me, the angle at the right side of the body
measured 96° in May 4th, but only 92.5° in June 9th. A
mistake due to posture is possible, so I waited for the imaging of the June
22nd. The angle was the same, so the pelvic tilt is actually reduced. I measured also a decrease in apparent curvature, first time after April 14th,
when it was 154°. This
time the angle of the curve measured 156°. Since there was
no improvement in May, I increased the
time wearing the corset. Again I wore
it at night and during the day,
several times even during walks, as at the beginning of therapy. New improvement shows that limits of the scoliosis
correction may have not been reached yet, while leveling of
the pelvis shows that my legs are not
really of unequal lengths or
the difference is very small. When I had to cross a
greater distance when walking down, I used to step
forward with my right foot, which
I could stretch more. I can now step forward with both feet, the difference in muscle and tendon tension
is gone. Asymmetry in raising straight legs is typical of
scoliosis (van Loon
2012). The circumference of my chest
is much larger now than it was at the beginning of treatment six years ago.
Best evidence for that are the underbust corsets I used then. In that time, I
tightened them almost to their maximum tightness. Now, I am not able to put
them on. In July 13th the curve measured
158°, a further improvement. But photographs made
on July 26th brought disappointment. The curve was 153° again. Two
days later I was able to derotate the chest with my hands and back muscles
only, what proves that it is flexible to some extent. In August 17th
the thoracic curve measured 156° and pelvic tilt 91°. |
||||||||
|
|
Pelvic tilt measured in August 17th.
Thumbs are put to the iliac crests of the pelvis to mark them. The angle at
the right side was 91°. |
|||||||
|
Dorsal and lateral views of
the state of scoliosis on September 12th 2012. |
||||||||
|
Is corset
harmful now? From April onwards, there was no real improvement of curvature. A few degrees better and then worse again, the situation remained unchanged on average. I found that the hump increases after wearing corset, several days without it improved the back. I've been watching what happens when I put on the corset. I found that the chest flattens, rotates. This has happened before, but only when I tightened corset too much. Now it happened already at a slight compression. It has become more flexible. I concluded that the therapy with corset is over, I should switch to exercises and other forms of chest derotation, which are more efficient at greater flexibility. Bodice has done its part, in the present state it does more harm than help. With the end of August 2012 I stopped
wearing corset. I straightened my back by frequently correcting posture and
by pressing the hump with my hands or the ground. On September 12th
thoracic curve measured 157°, less than on September 1st (153°), but equal to
the best achievements in the past. Later on, I tried to wear the corset again
occasionally and found it can be used again. During longer
interruption of wear the chest stabilized in the new, better position. |
||||||||
|
|
In a
view from the left side made on 1st November 2012 the restored
lumbar lordosis is seen well. Smaller picture at right, taken in August 2009,
shows a remarkable difference in the hump size and inclination of the back
plane. Since
lumbar lordosis was missing, the head is shifted forward, and back muscles
are strained as a result. |
|||||||
|
X-ray imaging According
to appearance the scoliosis improved substantially since the beginning of
treatment. The hump is markedly reduced, the curvature of the spine seems
to be reduced also. But only x-rays can show the true
state of the curves, so I was x-rayed on
October 8th. Images have
shown that in fact there has
been almost no change in spinal curvature. All I have
achieved is derotation of the chest, improvement of the shape of the ribs and
lumbar lordosis. This reduced the hump
and led to better
rib support of the right side of
the chest at front and left side in rear.
Changes have a positive effect on breathing and possibly prevent further deterioration of the curves. The curvature didn't improve, however, indicating independence of processes behind bending of the spine and rotation of the chest. Although the curvature did not reduce, the treatment was successful, as it improved performance and physical appearance. Physical appearance is the most common reason for which patients or their parents choose to have spinal surgery (Hawes 2003, 2006, 2010). In the treatment of scoliosis, attention is focused particularly on the curvatures, but derotation may be more important. Lung volume reduction, which can be life-threatening, is not caused by curvature of the spine, but rotation of the chest which becomes flattened. |
||||||||
|
|
X-ray image of the spine, performed
on October 8th 2012. If the curvature of more
than 100 degrees resulted from uneven bone growth, vertebrae should be
wedge-shaped. But no, only intervertebral discs, which are made of cartilage,
are transformed. They are stretched like bellows of an accordion. |
|||||||
|
Discussion A question
remains what is in the successful treatment of scoliosis that distinguishes
it from less successful established methods. The most
important difference is in
constant slight compression
of the chest by the corset. I believe it is
also important to create lumbar lordosis, thus to correct spinal curvature
forwards in the waist. To this end I have slightly adjusted the corset. The
lower tip of the front metal busk with staples I bent backwards. Thus I have
caused the pelvis to tilt forward and the lumbar lordosis to increase while
the pressure to the stomach decreased. Feeling of a hug given by the bodice is
pleasant. Absolutely it should not be tightened too much. If it starts to
pinch us, we must release the grip by loosening the lace at the back. This
allows us to constantly adapt corset to our body. The body changes with the
filling and emptying of the stomach and the degree of hydration. Corsets of textile embrace the whole body,
but the strongest pressure is directed on the most prominent angles of ribs
and pushes them inward. Since the bodice acts with the same force on the ribs
from the other side also, the ribs are slowly getting more rounded, gaining
the proper form. Thus the deformation of the chest is reduced. However, since
the corset does not have empty spaces where the chest could expand, treatment
with textile corset must be interrupted. Flat back is often accompanying scoliosis
(Negrini et al. 2012). It has the same shortcomings as the flat foot, it does
not allow flexibility. The spine should be slightly curved, so the creation
of correct lordosis is so important. When the spine is curved in the sagittal
plane, curves to the sides could be reduced (van Loon et al. 2008). In people without the lordotic curve the head
is not positioned above the pelvis, but in front
of it. The center of gravity outside
the body axis causes overload of back
muscles causing pain. Today, it seems incomprehensible that the first
Milwaukee braces were designed to reduce lordosis (Fayssoux et al. 2010). TLI
(Thoracolumbar Lordotic Intervention) brace, which is
symmetric and restores lordosis, is now tested in the Netherlands for the
treatment of adolescent scoliosis (van Loon
et al. 2012). A. Negrini
et al. (2008) showed it is possible to obtain a significant improvement of
scoliosis in adults with exercises. I am convinced
that wearing a backpack with camera equipment on my walks in nature was as
important for the treatment of scoliosis as wearing the corset, which shapes
the chest. Initially, I used them simultaneously, but later alternatingly,
what proved to be more effective. Backpack wear leads to strengthening of the
muscles that support the spine to stand upright. In addition, straps are
forcing my shoulders to be at the same height when wearing a backpack. Backpack with my camera
equipment weighs 3.5 kilograms
and my weight is 42-43 kg. So pack weighs 8.2% of
my weight. When I started going
on walks without the corset, a muscle started to ache on the left (concave)
side of the back, which was shortened due to scoliosis. But I persisted. If
pain was severe, I stopped for a rest and then went on. When the muscle was
strengthened the pain no longer occurred. After walking the hump increased
temporarily. But the strengthened muscles then straighten the back. We can
help by pressing the hump to the chair backrest while sitting or to the
ground when lying down. After the spine
bends sideways due to asymmetric posture or other reason, back muscles on the
convex side of the curve, which become stretched, cause rotation of the
vertebrae and ribs (Brodhurst 1855). The ribs are pulled back to create a
hump. This
explanation of chest rotation is forgotten now, but several facts speak in
its favour. Back muscles are even more tense when we
lean forward. The hump becomes larger and is seen even at slight curvatures.
Measurement of back tilt when bending forward has long been a test for the
presence of scoliosis, called the Adams test. The spinous processes which serve for the
attachment of muscles and ligaments are curved to the concave side in rotated
vertebrae, a clear sign they have been exposed to a prolonged stress. They
are linked together by the muscles, while vertebral bodies deviate easier
from the body axis. Derotation and diminished hump can be
achieved by the muscles on the concave side, when they are sufficiently
robust. This
fact is used by the physiotherapists to correct posture in scoliotic
patients. On repeated asymmetric loading, however,
vertebrae and ribs are transformed, making it difficult or
impossible to return to the initial state (Hawes &
O'Brien 2006). The
transformation of vertebrae and ribs in the process of bone remodeling is
regulated by several hormones. One of them is melatonin, secreted by the
pineal gland at night. In chickens and rats with destroyed pineal gland
scoliosis developed, but administration of the melatonin prevented that
(Acaroglu et al. 2012). It was suggested that lack of melatonin could be the
cause of idiopathic scoliosis in humans also. But such a shortage was not
detected in scoliotic patients (Brodner et al. 2000). Melatonin receptors can
be impaired (Man et al. 2011). Melatonin suppresses bone remodeling by
inhibition of bone resorption (Histing et al. 2012). When there is a shortage
of melatonin, bone remodeling accelerates. During bad posture, when bones are
loaded asymmetrically, scoliosis develops in children with rapid bone
remodeling. Melatonin secretion is stopped by light and magnetic fields. To
prevent scoliosis, children should sleep long enough in a dark room with
electronic devices turned off. Transient
melatonin deficiency is associated with curve progression and administration
of melatonin before sleep may prevent this (Machida et al. 2009). Leptin, secreted by adipose tissue, is also among the hormones suspected to have a role in the development
of scoliosis. Girls tend to have higher levels of leptin than boys because
they have more fat tissue. Fat
deposition is stimulated by the female
sex hormone estradiol (Burwell
et al. 2009). This
could be the reason why adolescent
scoliosis is much more common in
girls. In mice without front legs, which are
forced to walk on two, leptin increased incidence
of scoliosis (Wu et al. 2012). In
girls with adolescent scoliosis less leptin
content was observed in the blood, but increased effect of leptin in
the brain. Leptin does not
affect the bone directly,
but inhibits the production and secretion of the
neurotransmitter serotonin in the brain (Yadav et al. 2009).
The consequences of reduced secretion of serotonin are appetite loss, reduced self-confidence or a
feeling of security and increased
activity of the sympathetic nervous system, which releases noradrenalin. This prevents
the accumulation of bone mass, namely inhibits the second part of bone
remodeling, the formation of
new bone tissue, and favours bone resorption. The
activity of the sympathetic nervous
system produces a lightweight skeleton
with long limbs, such as prevalent in
girls with adolescent scoliosis. The level
of serotonin in the brain is not only affected by leptin, of course.
Uncertainty after diagnosis and the treatment for scoliosis can significantly
reduce adolescent self-esteem, increasing the activity of the sympathetic
nervous system, which can speed up the curving of the spine. The adolescent
needs professional support during treatment (Tavernaro et al. 2012). This gives
him a sense of security or, in other words, increases the activity of the
serotonergic neurons in the brain which also inhibit the perception of pain. The disadvantage of plastic braces, used for the treatment of scoliosis and which immobilize thorax, is the atrophy of muscles due to constant support of the brace. Rigid braces reduce the curvature of the spine, but when they are not worn any more, the curve increases again. Weakened muscles cannot keep the backbone in the upright position. A review by Fusco et al. (2011) showed that physical exercises can improve the curvature, strength, mobility and balance of patients with adolescent idiopathic scoliosis. Children
with scoliosis caused by a neurological deficit have weak muscles even
without a brace. They are treated in the U.K. by custom designed suits made of Lycra fabric with
pre-stressed elastic reinforcement panels which derotate the trunk and guide
patient into a proper posture (Matthews & Crawford 2006). Suits are
tested also in mild idiopathic scoliosis cases. Although corsets from textiles in the 19th
and the first half of the 20th century were sometimes used to
treat or at least alleviate scoliosis, they did not gain sympathy of the
leading physicians of the time. Albee (1919) published a picture of a textile
corset for the treatment of scoliosis, but he recommends
it only for immobilisation after spine surgery. The doctors
cited corset wear in young women of higher social classes as one of the main
causes of scoliosis, because it causes muscle atrophy. Absurd is that instead of textile corsets they
introduced treatment with plaster casts and rigid braces, which weaken
muscles just as much, if not more. Rigid braces for the treatment of scoliosis
were used first by Ambroise Paré (1510-1590). They were made of metal. Among
other things, he wrote that bracing does not help when the skeleton matures
and the growth stops (Fayssoux et al. 2010). This assertion has rarely been
contradicted. Brodhurst (1855) describes and figures a fairly successful treatment
of an 18-year-old girl with his supporting device, which was the precursor of
today's rigid braces and acted the same way. It put pressure on the convex
side of the curve and lifted the shoulder in the concave side, just like a
modern Chêneau brace made of plastic. Using traction and massage, Brooks,
Krupinski & Hawes (2009) were able to improve chest expansion and
decrease thoracic curvature in an adult with idiopathic scoliosis. Negrini et
al. (2008) hypothesize that improvement of adult scoliosis achieved by their
patient is a consequence of recovery from a postural collapse without changes
in bone structure. The treatment of severe scoliosis described
here denies the established belief that in adults an improvement cannot be
achieved with corsets. Actually, this should hold true also for most
adolescents in the time of growth. Guidelines of the SOSORT Society for the
treatment of idiopathic scoliosis from 2011 (Negrini et al. 2012) indicate
that the goal of treatment with braces is to halt curve progression at
puberty (or possibly even reduce it). It is believed that it is impossible to
fully eradicate scoliosis with conservative treatment (no surgery). However, by combining the use of
textile corsets, manipulation and
physiotherapy, chest derotation can be achieved which could prevent further progression of scoliosis. The spine could
not bend sideways, if ribs would not withdraw in the process of
chest rotation. After derotation ribs support
the spine and prevent further bending, they
serve as support beams. So
we can possibly avoid operations
that may have adverse consequences
because of the operation itself
or the fusion
of the vertebrae. Successful treatment of a single case does not mean that we can always expect the
same result. But even a single
successful treatment of an adult provides evidence that the premise about scoliosis
as irreversible process is wrong (Hawes
2003, 2006, 2010). If chest deformity can be reduced in a patient with severe scoliosis in adulthood, it is much
easier to do that in young patients in the period of rapid growth. Textile corset can
improve the shape of the ribs,
which cannot be done by a surgeon at
an operation. Lordotic curve of the lumbar spine is
also created, if not developed, and with this tension of the back muscles is
reduced. This reduces the possibility that muscles turn vertebrae and ribs,
to rotate them. Therapy with the corset may not be suitable for people with severely decreased lung function, because corset restricts breathing. But I did
not notice this at the beginning of treatment. My chest wall was probably so
rigid that wearing corset didn't make any difference. When I tried to
walk up a steep mountain path with the corset now, I found it unbearable.
Every few steps I had to stop to get breath. I already forgot that such was
my usual performance before the improvement of chest volume. To successfully derotate the chest additional
manipulative and physiotherapy is needed. My walks with backpack
were not intended to be part of the therapy, but they proved to be just that.
Postural corrections at any time during the day are also very important as
they eliminate unbalanced loading of the skeleton (Lehnert-Schroth 2007). I
added occasional pressure to the hump from behind, recommended also when
applying plaster cast as an effective treatment for scoliosis in young
children (D'Astous & Sanders 2007). Only derotation
of vertebrae and ribs reduces
the hump and increases volume
of the chest, thus improving
lung function. Surgeons only reduce the sideways
curvature of the spine in operation,
rotation of the chest persists and
hump may even increase.
To improve appearance, some surgeons
excise ribs that
form the hump and thus further impede breathing (Weiss &
Goodall 2008). A combination of chest compression by a
bending brace together with exercises is used in Brazil to treat scoliosis
(Haje et al. 2011). They use plastic braces made after plaster cast moulds.
The method is effective in compliant adolescent patients. The
effectiveness of a combination of exercises and wearing brace in adult
patients with scoliosis was reported by Papadopoulos (2013). The formation of idiopathic scoliosis is probably not initiated by
asymmetrical primary bone growth
in the growth plates
that exist only in children. Most spinal
deformities begin as a nonstructural scoliosis (Hawes &
O'Brien 2006). Wedge-shaped vertebrae
are not always present, in some cases only cartilaginous intervertebral discs
are transformed. Bending of the spine progresses even after
fusion of the vertebrae by surgery and may break the metal rods that should
keep it straight. All hormones, known to
have an impact on the development of
scoliosis affect bone remodeling which slows
down with adulthood, but never completely ceases.
Therefore, scoliosis usually progresses slowly
in adulthood. This gives us the opportunity to reverse the process – both in children and adults who
have at least some growth
hormone secretion. Aota et al. (2013) found an
increased amount of bone resorption marker in the majority of patients with
adolescent idiopathic scoliosis, while the bone formation marker was at a
normal level. Thus, in them bones degrade faster than regenerate. This decreases
the strength of the bone and can lead to osteoporosis, known to cause
scoliosis in the elderly. Heredity certainly influences the development of
scoliosis which often occurs in several family
members. However, the conclusion that the asymmetric growth
is genetically determined is incorrect. The
spine must be unevenly loaded first. Mice and rats used in research are
forced to walk on two legs to develop scoliosis. If
scoliosis depended on the genetic predisposition only, the amputation of
forelegs would not be necessary. The bone remodeling process is regulated by a series of hormones and the functioning
of hormones is dependent on their receptors. Genes regulate the production
of hormones and the formation of receptors. Because of them the bone remodeling proceeds faster
or slower. However, the genes
do not determine that the spine bends and
how it bends. This
depends on the posture, remodeling only allows the bone to adjust to the predominant posture. This is often useful, since the bones are strengthened where they are loaded and thus fractures are prevented,
while they become weaker where there
is no load. In the case of scoliosis the remodeling is harmful,
unfortunately. Vertebrae of curved spine are
constantly overloaded on the concave side, but in contrast to intermittent
loading, which strengthens bone, static loading does not stimulate bone
formation (Klein-Nulend et al. 2012). More attention should be directed to
the correct posture of children who are often hunched, or tilt sideways when
sitting in school or in front of computers. Scoliotic patients need to learn
upright stance, because feelings deceive them to think they are upright when
they tilt. But why most of the thoracic curvatures
are directed to the right and lumbar to the left? The spine is functional
only with its muscles and their role should be considered. Scoliosis
is more common in children who are engaged in certain sports. Modi et al.
(2008) found 6 children with thoracic or thoraco-lumbar curve greater than
10° among 116 volleyball players. 5.2% of players with scoliosis is much in
comparison with the control group, in which 1% of children had scoliosis. But
20 players (17%) had back tilted more than 5° when leaning forward (Adams
test) because of rotated ribs and vertebrae. This is due to better-developed
back muscles on the side where the hand with which they throw the ball is.
Mostly it is the right side, because right-handedness predominates over
left-handedness. Among players with scoliosis all right-handed players had
thoracic spine curvature directed to the right, the only left-handed player
to the left. Imbalanced muscle use may therefore initiate scoliosis by
rotation of the ribs and vertebrae. Bending of the thoracic spine to the
right in right-handers and to the left in left-handers follows because the
spine loses support from the ribs. Spinal curvature triggers the rotation of
vertebrae and ribs by the muscles and vice versa. This can
lead to a vicious cycle that increases the curvature. Goldberg & Dowling (1990) found statistically
significant correlation between scoliosis configuration and handedness in 254
girls with idiopathic scoliosis. The curve pattern matched handedness in 82%.
Of 228 right-handed children, 197 had a right convex curve pattern; of 26
left-handed children, 12 had a left convex pattern. Thus, asymmetrical use of thoracic muscles initiates scoliosis in a
large percentage of cases, but not all. Vertebral rotation was analyzed in the normal,
nonscoliotic thoracic spine of children aged 0 to 16 years by Janssen et al.
(2011). They have previously identified a rotational pattern in the normal
nonscoliotic adult spine that corresponds to the most common curve types in
adolescent idiopathic scoliosis. In infantile idiopathic scoliosis, curves
are typically left sided and boys are affected more often than girls, whereas
in adolescent idiopathic scoliosis, the thoracic curve is typically right
sided and predominantly girls are affected. Analysis
of the normal spine showed that the mid and lower thoracic vertebrae were
rotated to the left in infants (more pronounced in boys than in girls), were
not significantly rotated to either side in juveniles, and were rotated to
the right in adolescents. Well-known predominance of right-sided
thoracic curves in adolescent idiopathic scoliosis and left-sided curves in
infantile idiopathic scoliosis can be explained by the observed patterns of
vertebral rotation that preexist at the corresponding age. We can conclude that rotation of vertebrae usually predates
scoliosis formation and determines the direction of the primary curve. A relation between asymmetrical position of the
thoracic organs and vertebral rotation in the normal spine has been found by
Kouwenhoven et al. (2007). Slightly rotated vertebrae due
to internal organ loads can be turned further by the muscles to a degree when
a continuous deterioration starts by shear forces of the ribs. If joint
ligaments are not firm enough this happens easier. Scoliosis develops in
patients with congenital laxity of connective tissue (Bushell et al. 1979)
and also in children with idiopathic scoliosis joint hypermobility occurs
more frequently than in healthy controls (Czaprowski et al. 2011). Handedness is a decisive factor of vertebral rotation in older
children. Scoliosis without an obvious cause occurs only in humans. The
same is true also of handedness: lateralization has not evolved to a similar
degree in any other vertebrate. The influence of handedness on the curvature may be
mediated through posture. When one sits and writes with his right hand, he
often bends to the left. The same happens when we try to reach something high
above us with one hand. The spine bends to the opposite side and shoulder on
that side is lowered. When the chest is symmetric, the ribs push vertebrae
back to the midline and derotate them when we straighten from the bended
posture. But when the chest is structurally rotated, they cannot do that
entirely. The importance of equal support of the spine through the ribs
from both sides had been
proved with experiments. Resection of posterior ends of ribs
on one side induced progressive scoliosis in young animals. The spine curved to the side where
heads and necks of the
ribs had been removed (Piggott 1971). Rotation of vertebrae does not eliminate support from the ribs, but
ribs on the concave side push only vertebral
bodies toward the convex side
and ribs on the convex side
direct all their force to the vertebral processes. This causes additional turning of the
vertebrae and bending of the
spine toward the convex side. Infants and juveniles
are not involved in physical
activity in which only the dominant hand is used.
In them, another factor rotates vertebrae to the left. This could be the
diaphragm, which gives constant left side orientated torsion to the
upper lumbar spine (Jansen 1912, summarized in
van Loon 2012). Orthopaedists of today only try to stop
progression of scoliosis, but Bernard E. Brodhurst wrote in 1864: "Spinal
curvature is curable; but only when all the circumstances which gave rise to
it are taken into consideration." He already knew how rotation
develops and that bone remodeling is behind transformation of the vertebrae.
In 1855 he wrote: "Torsion or rotation of the vertebrae on their axes
having commenced, distortion proceeds more rapidly than heretofore...Tension
of the muscles on the side of the convexity is at the same time increased.
And these acting on the vertebrae, cause them to be twisted,—the spinous
processes towards the concavity, and the thickest portion of the bodies of
the vertebrae into the convexity of the curve: and, from continued pressure,
the bodies of the vertebrae themselves undergo partial absorption, and losing
something of their natural form, become wedge-shaped." He had an answer
to the problem: "...although the treatment required is prolonged,
rotation is overcome, when not extreme, in the same ratio as the lateral
inclination. This is facilitated by pressure made from behind forwards, on
the angles of the ribs." |
The Schroth Method: Exercises for Scoliosis Physical Therapy for Adolescents with Idiopathic
Scoliosis Medical and Commercial Supports for Scoliotic Patients, 1819-1935 Brodhurst,
Bernard Edward (1822 - 1900) Bone Turnover Markers
|
|||||||
|
|
The Van Winkle corset-brace for the
treatment of thoracolumbar scoliosis. Albee, 1919. |
|||||||
|
Left: Brodhurst's device for
the treatment of scoliosis; Middle: the same device in use (Brodhurst 1855);
Right: modern Chêneau brace acts by the same principle (Weiss & Weiss
2005). |
||||||||
|
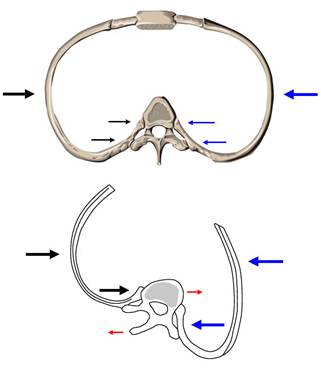
Ribs of a symmetric chest stabilize vertebrae and straighten the
spine (top). In a rotated chest (above) forces of the ribs turn vertebrae and
cannot prevent bending of the spine sideways. |
Extending to and hanging with the
left hand on barely accessible holds has proven to be the most effective
exercise for stretching the spine. If scoliosis is caused by the predominant
use of the right hand, it can be cured by frequent use of the left hand in
normal work and exercise. |
|||||||
|
Continuation of treatment In order to stretch the spine
and reduce side curvature, I included stretching exercises for the left side
of the body into the therapy in 2013. With left hand, I pushed at the hip
while standing or at the thigh while sitting and stretched the left side. I
lifted the body with my hands holding handles of a chair, and the spine
streched due to gravity. With my left hand, I stretched out to reach holds
above the door. The last exercise in particular has proven to be effective,
since the hump reduced during the exercise and the spine straightened
significantly. This confirms the theory that scoliosis develops due to
predominant use of the dominant hand, in my case right. Using the left hand
we oppose the forces that caused the curvature. Because
I can reach things above me easier, I concluded that the lateral
curvatures of the spine are more flexible.
Apparent curve on the photographs made in December 2013 measured
161°. But radiographs from
28 October 2014 showed that the curvature
didn't improve. Prognosis for most patients
with more than 100 degree curvature of the spine is
death in forties or fifties due to respiratory or heart failure, although there are
exceptions (Rom & Miller 1978). With my therapy I have tried to show that this
fate can be avoided without surgery. An
important difference exists between adult patients with scoliosis and children who are still growing. While vertebrae of an adult change
shape only with bone remodeling, in a child they grow
in length. Growth takes place with
ossification of cartilage in growth plates under the articulating surfaces. In the twisted spine unevenly loaded cartilage is compressed on the concave side and stretched on the convex side.
So the bone grows faster on the convex side of
the vertebrae which become wedge shaped (Aronsson & Stokes 2011). Effective
braces are those that reduce the
curvature of the spine and thereby eliminate uneven pressure on the cartilage. A few years ago there were not many studies that proved the
effectiveness of braces. The problem was to determine the real duration of brace wear.
This problem is now solved with temperature sensors inside the brace, showing
how many hours per day
the child really wears the brace, as it is effective only on the body. Weinstein
et al. (2013) have found that
brace prevents progression of adolescent idiopathic scoliosis if it is worn at least 13 hours a day. Results are better when brace
is worn over a longer time. 90% of children who wore a brace for at least 13 hours a day, have reached the end of
the growth period without the need
for surgery. Aulisa et al. (2014) found that brace
is very effective also in the treatment
of juvenile scoliosis. Curve correction was accomplished in 79% of patients, the curve stabilized in 16%, only in 6% progressed. Lusini et al.
(2013) have found that wearing a brace can reduce
the curvature even in patients with curve magnitude over 45° Cobb, who had refused
surgery. |
||||||||
|
The state of scoliosis on December
21st 2013. |
||||||||
|
References Acaroglu,
E., et al., 2012: The metabolic basis of adolescent idiopathic
scoliosis: 2011 report of the ‘‘metabolic’’ workgroup of the Fondation Yves
Cotrel. Eur. Spine J., 21: 1033–1042. Albee,
F. H., 1919: Orthopedic and Reconstruction Surgery,
Industrial and Civilian. W. B. Saunders Company, Philadelphia and London. Aota, Y., et al., 2013: Relationship
between bone density and
bone metabolism in adolescent idiopathic scoliosis (AIS). Scoliosis, 8
(Suppl. 2): O4. Aronsson,
D. D., I. A. F. Stokes, 2011: Nonfusion
treatment of adolescent idiopathic scoliosis by growth modulation
and remodeling. J. Pediatr. Orthop., 31 (1 Suppl): S99–106. Aulisa,
A. G., et al., 2014: Brace treatment in juvenile idiopathic scoliosis: a prospective study in accordance with the SRS criteria for bracing studies
- SOSORT award 2013 winner.
Scoliosis, 9: 3. Brodhurst,
B. E., 1855: On
Lateral Curvature of the Spine, its Pathology and
Treatment. John Churchill, London. Brodhurst,
B. E., 1864: Curvatures of the spine, their causes, symptoms, pathology and
treatment. John Churchill and sons, London. Brodner,
W., et al., 2000: Melatonin
and adolescent idiopathic
scoliosis. The Journal of Bone & Joint
Surgery, 82-B: 399-403. Brooks,
W. J., E. A. Krupinski, M. C. Hawes, 2009: Reversal
of childhood idiopathic scoliosis in an
adult, without surgery: a case report and literature review. Scoliosis,
4: 27. Burwell,
R. G., et al., 2009: Pathogenesis of adolescent idiopathic scoliosis in girls - a double neuro-osseous
theory involving disharmony between two nervous systems, somatic and
autonomic expressed in the spine and trunk: possible dependency on
sympathetic nervous system and hormones with implications for medical therapy.
Scoliosis, 4: 24. Bushell,
G. R., et al., 1979: The Collagen of the Intervertebral Disc in
Adolescent Idiopathic Scoliosis. The
Journal of Bone and Joint Surgery, 61-B (4):
501-508. Czaprowski, D., et al., 2011: Joint
hypermobility in children
with idiopathic scoliosis: SOSORT award 2011 winner. Scoliosis,
6: 22. D'Astous,
J. L., J. O. Sanders, 2007: Casting and Traction
Treatment Methods for Scoliosis. Orthopedic
Clinics of North America, 38: 477-484. Fayssoux,
R. S., et al., 2010: A History of Bracing
for Idiopathic Scoliosis in North America.
Clin. Orthop. Relat. Res., 468 (3): 654-664. Fusco, C., et
al., 2011: Physical
exercises in the
treatment of adolescent idiopathic scoliosis: An updated systematic review.
Physiotherapy Theory and Practice,
27 (1): 80–114. Goldberg, C., F. E. Dowling, 1990: Handedness and scoliosis convexity: a reappraisal. Spine, 15: 61-64. Haje, S. A., D. de
Podesta Haje, G. E. Vieira Martins, M. Goncalves Ferrer, 2011: The spine lateral bending and the
dynamic chest compression principles for concomitant orthotic treatment of
scoliosis and pectus deformities. Coluna/Columna, 10 (4): 293-299. Hawes, M. C., 2003, 2006,
2010: Scoliosis and the Human Spine. A Critical Review of Clinical Approaches
to Treatment of Spinal Deformity in the United States, and A Proposal for
Change. Tucson Arizona, U.S.A., 176 pp. Hawes, M. C., J. P. O'Brien, 2006: The
transformation of spinal curvature into spinal deformity: pathological processes and
implications for treatment. Scoliosis, 1: 3. Histing, T., et al., 2012: Melatonin
impairs fracture healing by suppressing
RANKL-mediated bone remodeling. Journal of Surgical Research, 173 (1): 83-90. Janssen, M. M., et al., 2011: Analysis
of preexistent vertebral rotation in the normal infantile, juvenile, and
adolescent spine. Spine, 36 (7): E486-491. Klein-Nulend, J., et al.,
2012: Mechanical loading and how it affects bone cells:
The role of the osteocyte cytoskeleton in maintaining our skeleton.
European Cells and Materials, Vol. 24 : 278-291. Kouwenhoven
J. W., et
al., 2007: The relation between organ anatomy and pre-existent vertebral rotation
in the normal spine: magnetic resonance imaging study in humans with situs
inversus totalis. Spine, 32 (10): 1123-1128. Lehnert-Schroth, C., 2007:
Three-dimensional treatment for scoliosis. A physiotherapeutic method for
deformities of the spine. The Martindale Press Palo Alto, California, 276 pp. Loon, P. J. M. van, 2012: Scoliosis Idiopathic? The
Etiologic Factors in Scoliosis Will Affect Preventive and Conservative
Therapeutic Strategies. In: Grivas,
T. B.: Recent Advances in Scoliosis. InTech, str. 211-234. Loon, P. J. van, B. A.
Kühbauch, F. B. Thunnissen, 2008: Forced
lordosis on the thoracolumbar junction can correct coronal plane deformity in adolescents with
double major curve pattern idiopathic scoliosis. Spine, 33 (7):
797-801. Loon, P. J. M. van, M.
Roukens, J. D. J. Kuit, F. B. T. M. Thunnissen,
2012: A new
brace treatment similar for adolescent
scoliosis and kyphosis based on restoration of thoracolumbar lordosis.
Radiological and subjective clinical results after at least one year of
treatment. Scoliosis, 7: 19. Lusini,
M., et al., 2013: Brace
treatment is effective in
idiopathic scoliosis over 45°: an observational prospective cohort controlled study. The Spine Journal, doi:
10.1016/ j.spinee.2013.11.040. Machida,
M., et al., 2009: Serum melatonin levels in adolescent idiopathic
scoliosis prediction and prevention for curve progression―a prospective
study. Journal of Pineal Research, 46 (3): 344–348. Man, G. C., et al., 2011: Abnormal
melatonin receptor 1B expression in osteoblasts from girls with adolescent
idiopathic scoliosis. Journal of Pineal Research, 50 (4): 395-402. Marty-Poumarat,
C., et al., 2007: Natural History of Progressive Adult Scoliosis.
Spine, 32 (11): 1227-1234. Matthews, M., R. Crawford,
2006: The
use of dynamic Lycra orthosis in the treatment of scoliosis: A
case study. Prosthetics and Orthotics
International, 30 (2): 174-181. Modi, H., et al.,
2008: Muscle Imbalance in Volleyball Players Initiates Scoliosis in Immature
Spines: A Screening Analysis. Asian Spine Journal, 2 (1): 38-43. Mohar, J., 2012: Untreated Early Onset Scoliosis - The Natural
Progression of a Debilitating and Ultimately Deadly Disease. In: Grivas,
T. B.: Recent Advances in Scoliosis. InTech, pp. 311-328. Negrini,
A., et al., 2008: Adult
scoliosis can be reduced through specific SEAS exercises: a case report.
Scoliosis, 3: 20. Negrini,
S., et al., 2012: 2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of
idiopathic scoliosis during growth. Scoliosis, 7 (3): 1-35. Papadopoulos, D., 2013: Adult
scoliosis treatment combining brace and exercises. Scoliosis, 8 (Suppl. 2): O8. Pearson, O. M.,
D. E. Lieberman, 2004: The Aging of
Wolff’s “Law”: Ontogeny and Responses to Mechanical
Loading in Cortical Bone. Yrbk. Phys. Anthropol., 47: 63–99. Piggott, H., 1971: Posterior rib resection in scoliosis. A preliminary report. J. Bone Joint Surg., 53 B: 663-671. Rom, W. N.,
A. Miller,
1978: Unexpected longevity in patients with severe kyphoscoliosis.
Thorax, 33: 106-110. Tavernaro, M., et al., 2012: Team care to cure adolescents with braces (avoiding low quality of life,
pain and bad compliance): a case–control retrospective study. 2011 SOSORT
Award winner. Scoliosis, 7: 17. Vasiliadis, E. S., et al.,
2009: Historical
overview of spinal deformities in ancient Greece. Scoliosis, 4:
6. Weinstein, S. L., L. A.
Dolan, K. F. Spratt, K. K. Peterson, M. J. Spoonamore, I. V. Ponseti, 2003: Health and Function
of Patients With Untreated Idiopathic Scoliosis. A 50-Year Natural
History Study. JAMA, 289 (5): 559-567. Weinstein,
S. L., et al., 2013: Effects
of Bracing in Adolescents with Idiopathic Scoliosis. New Engl. J. Med., 369: 1512-1521. Weiss, H. R., D. Goodall, 2008: Rate
of complications in scoliosis surgery – a
systematic review of the Pub Med literature. Scoliosis, 3: 9. Weiss, H. R., G. M. Weiss,
2005: Brace treatment during pubertal growth spurt in girls
with idiopathic scoliosis (IS): A prospective trial comparing two different
concepts. Pediatric Rehabilitation, 8(3):
199–206. Wu, T., et
al., 2012: Role
of high central leptin activity in a scoliosis model created in bipedal
amputated mice. Research
Into Spinal Deformities 8, Studies in
health technology and informatics, 176: 31-35. Yadav,
V. K., F. Oury, N. Suda, Z-W. Liu, X-B. Gao, C.
Confavreux, et al.,
2009: A Serotonin-Dependent Mechanism Explains the Leptin Regulation
of Bone Mass, Appetite, and Energy Expenditure. Cell,
138: 976–989. |
||||||||